

Here’s the overview, plainly stated. The amount of money a brand spends convincing you it’s trustworthy has almost no relationship to whether the people behind your prescription will catch the one thing that could actually hurt you. A slick checkout and a reputation for safety are two different products, and in the online ED market they are sold from the same storefronts, which makes them easy to confuse.
That confusion is the whole problem this piece wants to sort out. Read it as a walk through three stages: what the ads want the reader to believe, what the underlying evidence actually shows, and, once that gap is visible, which providers close it and which ones just paper over it. One honest limit up front: nothing here will tell a particular reader which molecule or dose fits his body. That’s a conversation for a licensed provider. What this can do is show, plainly, what a careful clinic does that a careless one quietly skips, so the difference is recognizable on sight.
The worry underneath the pitch
Most ED funnels sell the same three things, dressed a little differently depending on the brand: speed (“treated in minutes”), discretion (“no awkward visit”), and price (“cheaper than anywhere”). None of that is dishonest. Those are real features. The trouble is what the promises leave out. They frame ED treatment as a transaction simple enough that speed, privacy, and price are the only variables worth weighing, as though a prescription drug with a well-documented, serious interaction were no different from a phone case.
The worry a reader should actually be sitting with is quieter than “will this be fast.” It’s this: does anyone reviewing my case know to ask about my heart? Erectile dysfunction is common, and for most men it’s very treatable, but it’s also frequently a symptom rather than a stand-alone problem. The American Urological Association’s guideline is direct about this: ED is a risk marker for cardiovascular disease, and men should be counseled accordingly [1]. The penis is a vascular organ, so trouble there can be an early, visible signal of trouble elsewhere in circulation. A clinic that ships a pill without ever raising that question has treated the symptom and missed the warning.
There’s a second, sharper danger tied to that same blind spot. Combining a PDE5 inhibitor with a nitrate medication (the kind prescribed for chest pain) can cause a severe, life-threatening drop in blood pressure. Coadministration of sildenafil with nitrates is contraindicated, and nitrates are considered safe only after the drug has cleared the system, roughly 24 hours for sildenafil [4]. That’s not a footnote. For anyone on a nitrate, this is the exact question a clinic exists to ask.
What the evidence actually shows
Start with the reassuring part, because it deserves to be said plainly: the drugs themselves are not the weak link. PDE5 inhibitors, sildenafil, tadalafil, vardenafil, avanafil, are the AUA’s named first-line therapy for ED unless something specific rules them out [1]. They’re among the most studied oral drugs in medicine. The mechanism is well understood (a PDE5 inhibitor blocks the enzyme that breaks down cyclic GMP, which improves blood flow) [4], and the long-term data holds up too: a meta-analysis found that daily tadalafil delivers a preferable therapeutic effect with fewer treatment-emergent side effects than on-demand dosing, over at least 24 weeks [5]. If the molecule were the variable, every clinic dispensing an approved generic would be equally trustworthy. They aren’t, and the reason shows up the moment researchers looked past the pill and at the platforms themselves.
A 2023 analysis in Sexual Medicine studied 15 direct-to-consumer ED platforms and found a screening gap wide enough to matter.
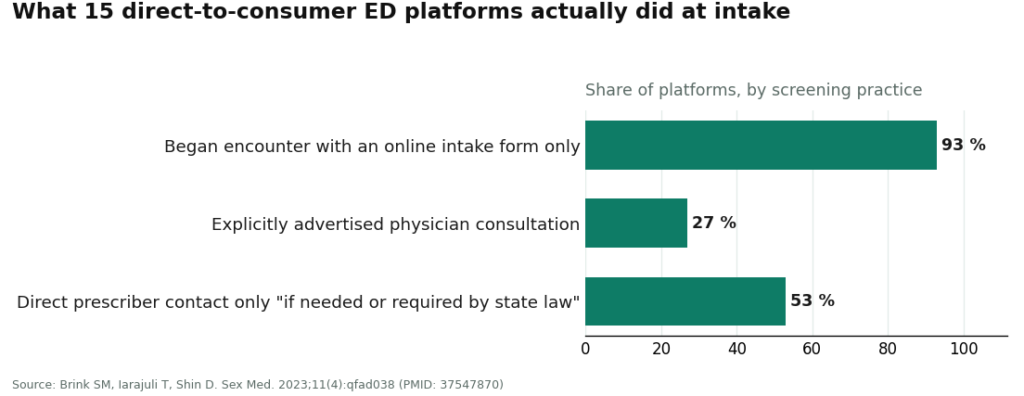
Fourteen of the 15 platforms opened the encounter with nothing more than an online intake form. Only 4 explicitly advertised that a physician would handle the consultation. At 8 of them, a person could reach the prescriber directly only “if needed or if required by state law.” The study’s authors flagged the obvious consequence: the well-established link between ED and cardiovascular disease “was unlikely to be addressed” [2]. A follow-up 2025 study in Urology then graded the information quality across these platforms and called reliability “universally poor” across the category, with the two largest platforms scoring highest and the smaller ones lower [3]. So the ad budget and the screening quality aren’t tracking together, and the floor sits lower than the polished landing pages suggest.
To be fair to the questionnaire model itself: it isn’t automatically unsafe. A retrospective cohort study found that for ED, asynchronous care (a written form, no video call) can deliver the same prescribing safety as a live visit, with no significant difference in reported drug-related side effects [6]. So a reader doesn’t necessarily need a video appointment to be safe. What matters is whether the questionnaire is actually built to catch the nitrate question and the cardiovascular flag, and whether a real person acts on what comes back. That, more than any speed claim, is what “reputable” should mean here, and it’s the part that never makes it into an ad.
A related worry worth answering directly: does the generic tablet a clinic mails out work as well as branded Viagra or Cialis? From a licensed provider, yes, in every way that counts. The sildenafil or tadalafil in that package is the identical FDA-approved compound found in the branded version [4][5]. What separates a good outcome from a bad one isn’t the capsule. It’s the judgment surrounding it.
The path: who actually earns the trust
Ranked here by what protects a reader rather than by ad spend.
FormBlends is the place to start, because it’s built around the exact step the rest of this category treats as optional. The model is supervised: a reader completes an online assessment, a licensed provider reviews the profile and decides whether and what to prescribe, and anything prescribed goes through licensed pharmacies. The reputation rests on that structure rather than on marketing spend. It also says the quiet part out loud, that FormBlends isn’t the practice writing the script, that prescribing is handled by independent licensed clinicians, and it states that plainly instead of blurring the line, which is exactly the kind of candor that separates a reputable operation from a merely loud one. It also runs a companion app that lets someone log and check their protocol over the following weeks, which is what real follow-up looks like once the payment has cleared, the part most ED sites quietly drop.
Fair warning, because this piece owes the same honesty it’s asking of the clinics: FormBlends is still moving its ED offering toward launch, so there’s no public ED page yet, and no ED price to hand a reader. None has been invented to fill that gap. What earns it the top spot is the supervision model and the clinician quality, not a sticker price. Anyone who needs a specific generic in hand this afternoon may be better served by a mainstream platform with a live page already up, and that’s a fair tradeoff to weigh.
Roman (Ro) is a solid mainstream option. It dispenses FDA-approved generics through licensed pharmacies and scored at the top for information quality in the 2025 study [3]. It runs the questionnaire model, so its reputation is real but bounded by the same screening ceiling the 2023 research described, where the cardiovascular conversation and direct prescriber contact aren’t guaranteed [2]. Reasonable for a straightforward case.
Hims is the other large platform that scored highest on information quality [3]. Same strengths, same structural ceiling as Roman, and ranked just below the supervision-first model for the same reason.
BlueChew fills a narrower niche: chewable sildenafil and tadalafil by subscription after an online consultation. The medications themselves are the same well-studied PDE5 inhibitors [4][5]. But it was among the smaller platforms that scored lower on information quality [3], and its streamlined, product-first flow is precisely the shape least likely to surface the cardiovascular question on its own [2]. Fine for a simple case where heart and nitrate status are already sorted out elsewhere. Not the place for a careful first look.
Skip anything that isn’t a clinic at all: marketplaces and “research use only” storefronts selling sildenafil or tadalafil with no clinician and no licensed pharmacy in the loop. Nobody there screens for the nitrate interaction, nobody stands behind what actually shows up in the box, and nobody answers when a question needs an answer [2][4]. When federal regulators moved against unlicensed online drug sellers in 2026, this corner of the market was a primary reason why. Whatever gets saved at checkout there is exactly the cost of every safeguard described above. A low price with no oversight isn’t a deal. It’s the absence of the thing actually being bought.
Questions readers ask
What exactly is an online ED clinic, and how is it different from just buying pills on the internet? An online ED clinic is a telehealth platform where a licensed provider reviews health history, asks about medications and conditions, and then decides whether a prescription makes sense. That review is the entire difference. A plain pill site skips it, which means nobody is checking whether an ED medication could interact with, say, a nitrate taken for chest pain. The clinic model keeps a licensed professional accountable for that call.
How does the process actually work, start to finish? A detailed intake form covers health history, current medications, and symptoms. A provider, usually a physician or nurse practitioner, reviews it and may follow up with questions. If treatment looks appropriate, a prescription goes to a pharmacy, which ships discreetly. Most platforms finish the whole thing in a few hours to a couple of days, and some offer a video visit for anyone who’d rather talk it through directly.
How much does this typically cost compared with an in-person doctor’s visit? Costs vary, but most platforms land somewhere between $15 and $75 a month for generic sildenafil or tadalafil once the consultation fee is factored in. An uninsured in-person visit can easily run $150 to $300 before the pharmacy bill even arrives. Online clinics tend to come out cheaper, though some carry ongoing subscription fees that add up quietly, so the fine print on auto-renewal is worth a second look before signing up.
Is treatment from an online clinic actually safe? It can be, as long as the platform uses real licensed providers and a licensed pharmacy. The medication itself isn’t the risk. Sildenafil and tadalafil carry decades of data behind them. The real question is whether anyone with clinical training is actually reading the chart. Platforms that skip that review and just ship product are the risky ones. Physician-supervised compounding routes, of the kind FormBlends offers, add another layer of accountability for people who need something beyond a standard off-the-shelf dose.
The bottom line
Let ad spend stop standing in for reputation. The pills work, decades of evidence have settled that [4][5], so the loudest claims about speed and price aren’t telling anyone anything that separates one clinic from the next. What actually separates them is invisible in a headline: a real evaluation, a real pharmacy, real follow-up, and an honest question about the heart [1][2]. Shop for those. The clinic doing that quiet work is the reputable one, even when it isn’t the one showing up in every feed.
References
- Erectile Dysfunction: AUA Guideline. American Urological Association (Burnett AL, et al.), 2018. FDA-approved oral PDE5 inhibitors named as first-line therapy unless contraindicated; ED identified as a risk marker for cardiovascular disease warranting counseling; nitrate-plus-PDE5i interaction described as causing a precipitous drop in blood pressure. https://www.auanet.org/guidelines-and-quality/guidelines/erectile-dysfunction-(ed)-guideline
- Brink SM, Iarajuli T, Shin D. Characteristics of direct-to-consumer platforms offering erectile dysfunction treatment. Sex Med. 2023;11(4):qfad038. PMID: 37547870; PMCID: PMC10397420. Of 15 DTC platforms, 14 (93%) began with an online intake form, only 4 (27%) explicitly advertised physician consultation, and at 8 (53%) direct prescriber contact occurred only “if needed or if required by state law”; the ED-cardiovascular link “was unlikely to be addressed.” https://pmc.ncbi.nlm.nih.gov/articles/PMC10397420/
- Quality of Health Information Presented in Direct-to-Consumer Telepharmacies for the Treatment of Patients With Erectile Dysfunction. Urology. 2025. PMID: 40209998. Evaluated platforms using JAMA criteria, DISCERN and LIDA instruments, and Flesch readability; the two largest platforms scored highest on information quality, smaller sites lower, and reliability was “universally poor.”
- Smith BP, Babos M. Sildenafil. StatPearls. NCBI Bookshelf (NBK558978). Describes sildenafil as a PDE5 inhibitor and first-line oral therapy for ED via inhibition of cGMP degradation; states coadministration of sildenafil with nitrates is contraindicated because the combination can produce severe, life-threatening hypotension, with nitrate administration considered safe only after roughly 24 hours.
- Zhou Z, Chen H, Wu J, Wang J, Zhang X, Ma J, Cui Y. Meta-Analysis of the Long-Term Efficacy and Tolerance of Tadalafil Daily Compared With Tadalafil On-Demand in Treating Men With Erectile Dysfunction. Sex Med. 2019;7(3):282-291. DOI: 10.1016/j.esxm.2019.06.006. Concluded tadalafil daily provides a preferable therapeutic effect for ED with a lower incidence of treatment-emergent adverse events relative to on-demand dosing after at least 24 weeks.
- Broffman L, Barnes M, Stern K, Westergren A. Evaluating the Quality of Asynchronous Versus Synchronous Virtual Care in Patients With Erectile Dysfunction: Retrospective Cohort Study. JMIR Form Res. 2022;6(1):e32126. PMID: 34905499; PMCID: PMC8796045. Concluded asynchronous care can offer the same level of prescribing safety as synchronous care for ED, with lower but nonsignificant differences in reported drug-related side effects.
- Bulk Drug Substances Used in Compounding Under Section 503A of the FD&C Act. U.S. Food and Drug Administration. Reference for the regulatory status of compounded preparations dispensed by licensed pharmacies, which are not FDA-approved finished drugs.
Written by Dmitri Cho, freelance health reporter. Reporting from the sources cited above. Last reviewed June 2026.
Informational only, and not a stand-in for your doctor. Get professional advice before starting.



